By Stephen Engelberg for ProPublica
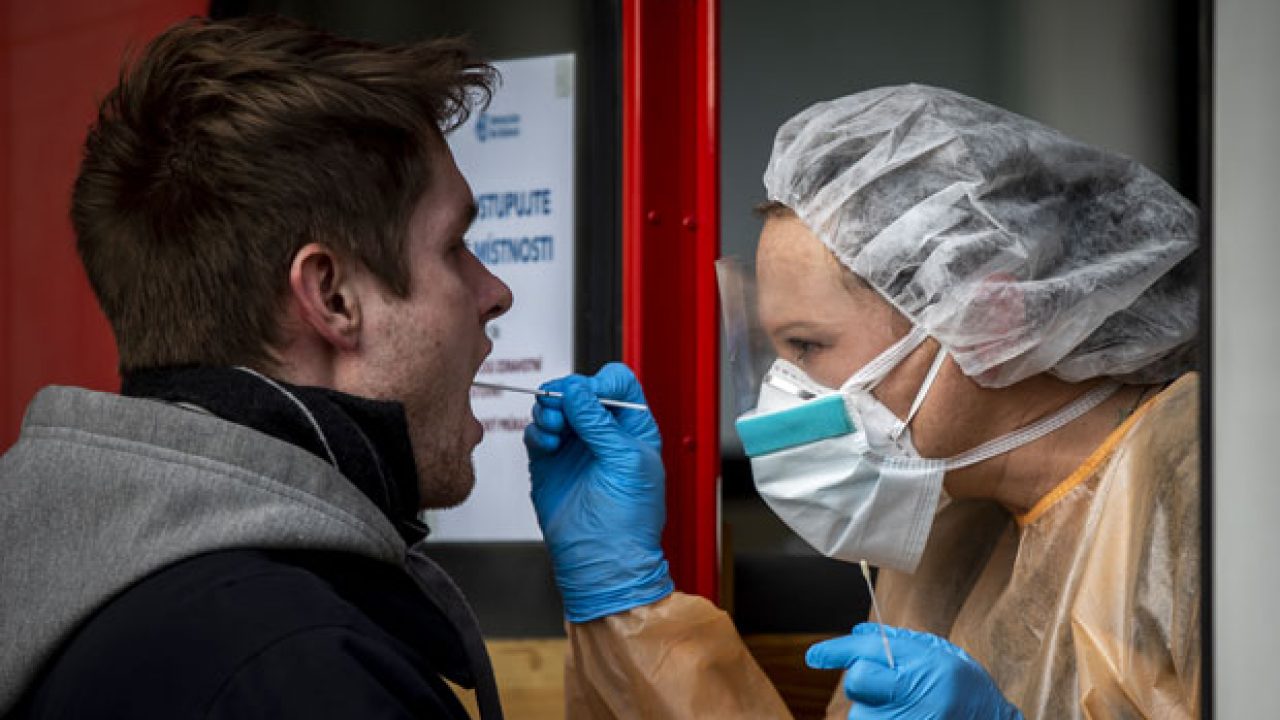 |
| This photo explains the problem in a nutshell. Not only are there not enough kits to meet demand, but the facemask, gown and gloves this health worker wears are also in short supply. Note that she is not wearing a face shield even though her eyes are a major route of exposure. (Photo from KTAR.com) |
Yet New York City, the epicenter of the outbreak in the U.S., has ordered doctors not to test anyone who is “mild to moderately ill” with COVID-like symptoms, a position also taken by Los Angeles.
As New York’s Health Department succinctly put it: “Outpatient testing must not be encouraged, promoted or advertised.”
Dr. Tom Frieden, former health commissioner of New York City and former head of the Centers for Disease Control and Prevention, said both viewpoints make sense.
“Where you stand depends on where you sit,” Frieden said. “Local context is all important. In New York City, today, you should not get tested if you have mild symptoms.”
The reason, he said, is that the health care systems in places like New York, Los Angeles and Seattle are about to be overwhelmed by a wave of people seriously ill from COVID-19. They know it’s coming.
Administering each test takes up protective gear, swabs and health care workers’ time, all of which should be reserved for patients with life-threatening conditions. On Monday, for instance, NewYork-Presbyterian Hospital reported that it had more than 600 patients with COVID-19.
Conversely, Frieden and other experts pointed out, the United States will need to pursue a policy of very broad testing if it hopes to slow the spread of the disease and restart parts of the economy anytime soon.
Frieden noted that one of the countries most effective in lowering its infection rate, Singapore, had great success in tracing and isolating the contacts of each infected person. That is no longer possible in New York state, which has reported more than 20,000 positive tests and has many times that number of people infected. But he said it remains doable in many other cities and towns.
“In places where you’ve got the cases way down, or there are no cases,” he said, “aggressive testing will be needed.”
The lack of testing continues to be a source of deep frustration across the country, with worried patients unable to find out whether they have the ordinary flu, the coronavirus or something else entirely. The availability of testing in regions that aren’t hot spots still faces an array of bottlenecks, from shortages of cotton swabs to the capacity of the labs processing the tests.
Dr. Scott Gottlieb, the former head of the Food and Drug Administration under President Donald Trump, argued in a widely read Twitter commentary for a multipronged approach to fighting the virus, which will involve overcoming all of these hurdles and significantly stepping up testing nationwide.
The current “shelter in place” orders, which have tens of millions of people in New York, California and other states limited to their homes and not going to work, he said, will ultimately have to be supplanted by a more targeted approach.
To do this, he wrote, the United States “must widely test our population” and “diagnose mild and even asymptomatic cases” with reliable tests that can be administered in doctors’ offices. “We must have tools to identify and isolate small outbreaks so we can lean less heavily” on locking down whole swaths of society, Gottlieb wrote.
Trevor Bedford, a University of Washington virologist who has been directly involved in detecting and fighting his state’s outbreak, offered a similar prescription in a recent series of tweets.
Bedford’s observations were prompted, in part, by a recent study by epidemiologists at Imperial College London that said countries had little alternative to maintaining strict restrictions on social contact until a vaccine is available, a process that could take 18 months.
The study forecast as many as 1.1 million to 1.2 million deaths in the United States if officials backed off the sorts of measures taken by New York and California in recent days.
Bedford said he was not that “pessimistic,” and he called for a strategy that “revolves around a massive rollout of testing capacity.” Recent studies, he wrote, support the argument that a “significant” portion of the transmission of the virus arises from people who spread it before they feel sick. There also are people who infect others while never experiencing any symptoms of their own.
Something approaching universal testing would make it possible to significantly reduce such “transmission routes.”
“If someone can be tested early in their illness before they show symptoms,” Bedford wrote, “they could effectively self isolate and reduce onward transmission compared to isolation when symptoms develop.”
He envisaged a future in which swabs are delivered to people’s homes for quick return and in which drive-through testing is widely available to anyone with a car. “There are logistics involved in getting a result quickly,” he wrote, “but it’s really just logistics, which can be solved.”
Bedford suggested an approach that appears to have worked in South Korea, which combined test results with “cell phone location data” on known positive cases, allowing notification of people who have been in proximity to confirmed cases to “self isolate and get tested.”
A third pillar of Bedford’s approach is a medical exam that does not yet exist — a blood test that can detect the presence of antibodies to COVID-19. Antibodies are created when the immune system successfully fights off an infection and people with them are “highly likely to possess immunity” and can “fully return to the workforce and keep society functioning.”
That assumption, like many about the virus, remains the subject of research. For his part, Frieden said he was cautious about taking any action based on a test that detects antibodies. Does it mean the person is immune from a second infection? “We can’t count on that,” he said. “We don’t yet know that.”
The clash between the short-term and long-term views of testing were on vivid display in the press conference last week that made headlines for Trump’s angry outburst at an NBC reporter.
Earlier in the briefing, Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases at the National Institutes of Health, sought to distinguish between the ultimate need for more tests with the immediate requirement that Americans stop gathering in workplaces, bars, streets and restaurants.
The extreme steps taken by California and New York, Fauci said, are “how you put an end to this outbreak.”
“Testing is important,” he said. “But let’s not conflate testing with the action that we have to take. Whether or not you test, do this. I’m not putting down testing as an important issue, but people seem to link them so much that if you don’t have universal testing, you can’t respond to the outbreak. You really can.”
Trump disparaged the notion of widespread testing as imagined by Bedford and others. “We don’t want every American to go out and get a test. Three hundred and fifty million people,” Trump said.
“We don’t want that. We want people that have a problem, that have a problem with they’re sneezing, they’re sniffling, they don’t feel good, they have a temperature.”
ProPublica is a Pulitzer Prize-winning investigative newsroom. Sign up for The Big Story newsletter to receive stories like this one in your inbox.
As New York’s Health Department succinctly put it: “Outpatient testing must not be encouraged, promoted or advertised.”
Dr. Tom Frieden, former health commissioner of New York City and former head of the Centers for Disease Control and Prevention, said both viewpoints make sense.
“Where you stand depends on where you sit,” Frieden said. “Local context is all important. In New York City, today, you should not get tested if you have mild symptoms.”
The reason, he said, is that the health care systems in places like New York, Los Angeles and Seattle are about to be overwhelmed by a wave of people seriously ill from COVID-19. They know it’s coming.
Administering each test takes up protective gear, swabs and health care workers’ time, all of which should be reserved for patients with life-threatening conditions. On Monday, for instance, NewYork-Presbyterian Hospital reported that it had more than 600 patients with COVID-19.
Conversely, Frieden and other experts pointed out, the United States will need to pursue a policy of very broad testing if it hopes to slow the spread of the disease and restart parts of the economy anytime soon.
Frieden noted that one of the countries most effective in lowering its infection rate, Singapore, had great success in tracing and isolating the contacts of each infected person. That is no longer possible in New York state, which has reported more than 20,000 positive tests and has many times that number of people infected. But he said it remains doable in many other cities and towns.
“In places where you’ve got the cases way down, or there are no cases,” he said, “aggressive testing will be needed.”
The lack of testing continues to be a source of deep frustration across the country, with worried patients unable to find out whether they have the ordinary flu, the coronavirus or something else entirely. The availability of testing in regions that aren’t hot spots still faces an array of bottlenecks, from shortages of cotton swabs to the capacity of the labs processing the tests.
Dr. Scott Gottlieb, the former head of the Food and Drug Administration under President Donald Trump, argued in a widely read Twitter commentary for a multipronged approach to fighting the virus, which will involve overcoming all of these hurdles and significantly stepping up testing nationwide.
The current “shelter in place” orders, which have tens of millions of people in New York, California and other states limited to their homes and not going to work, he said, will ultimately have to be supplanted by a more targeted approach.
To do this, he wrote, the United States “must widely test our population” and “diagnose mild and even asymptomatic cases” with reliable tests that can be administered in doctors’ offices. “We must have tools to identify and isolate small outbreaks so we can lean less heavily” on locking down whole swaths of society, Gottlieb wrote.
Trevor Bedford, a University of Washington virologist who has been directly involved in detecting and fighting his state’s outbreak, offered a similar prescription in a recent series of tweets.
Bedford’s observations were prompted, in part, by a recent study by epidemiologists at Imperial College London that said countries had little alternative to maintaining strict restrictions on social contact until a vaccine is available, a process that could take 18 months.
The study forecast as many as 1.1 million to 1.2 million deaths in the United States if officials backed off the sorts of measures taken by New York and California in recent days.
Bedford said he was not that “pessimistic,” and he called for a strategy that “revolves around a massive rollout of testing capacity.” Recent studies, he wrote, support the argument that a “significant” portion of the transmission of the virus arises from people who spread it before they feel sick. There also are people who infect others while never experiencing any symptoms of their own.
Something approaching universal testing would make it possible to significantly reduce such “transmission routes.”
“If someone can be tested early in their illness before they show symptoms,” Bedford wrote, “they could effectively self isolate and reduce onward transmission compared to isolation when symptoms develop.”
He envisaged a future in which swabs are delivered to people’s homes for quick return and in which drive-through testing is widely available to anyone with a car. “There are logistics involved in getting a result quickly,” he wrote, “but it’s really just logistics, which can be solved.”
Bedford suggested an approach that appears to have worked in South Korea, which combined test results with “cell phone location data” on known positive cases, allowing notification of people who have been in proximity to confirmed cases to “self isolate and get tested.”
A third pillar of Bedford’s approach is a medical exam that does not yet exist — a blood test that can detect the presence of antibodies to COVID-19. Antibodies are created when the immune system successfully fights off an infection and people with them are “highly likely to possess immunity” and can “fully return to the workforce and keep society functioning.”
That assumption, like many about the virus, remains the subject of research. For his part, Frieden said he was cautious about taking any action based on a test that detects antibodies. Does it mean the person is immune from a second infection? “We can’t count on that,” he said. “We don’t yet know that.”
The clash between the short-term and long-term views of testing were on vivid display in the press conference last week that made headlines for Trump’s angry outburst at an NBC reporter.
Earlier in the briefing, Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases at the National Institutes of Health, sought to distinguish between the ultimate need for more tests with the immediate requirement that Americans stop gathering in workplaces, bars, streets and restaurants.
The extreme steps taken by California and New York, Fauci said, are “how you put an end to this outbreak.”
“Testing is important,” he said. “But let’s not conflate testing with the action that we have to take. Whether or not you test, do this. I’m not putting down testing as an important issue, but people seem to link them so much that if you don’t have universal testing, you can’t respond to the outbreak. You really can.”
Trump disparaged the notion of widespread testing as imagined by Bedford and others. “We don’t want every American to go out and get a test. Three hundred and fifty million people,” Trump said.
“We don’t want that. We want people that have a problem, that have a problem with they’re sneezing, they’re sniffling, they don’t feel good, they have a temperature.”
ProPublica is a Pulitzer Prize-winning investigative newsroom. Sign up for The Big Story newsletter to receive stories like this one in your inbox.